The Health Economics of Global HPV Screening: A Blueprint for the 2030 Elimination Goals
As the world unites around International Women’s Health Day on May 18, the WHO’s 2030 strategy to eliminate cervical cancer stands as both a moral mission and one of the most compelling economic growth strategies of the decade.
As the global community unites around International Women’s Health Day on May 18, a critical focal point emerges in the fight for health equity: the World Health Organization’s (WHO) 2030 strategy to eliminate cervical cancer. This historic initiative is anchored by the ambitious “90-70-90” targets—vaccinating 90% of girls by age 15, screening 70% of women with high-performance tests by ages 35 and 45, and treating 90% of identified pre-cancers and cancers.
Beyond the profound human impact, achieving these targets is a highly lucrative macroeconomic imperative. This article explores the transformative health economics of primary HPV screening, its superiority in clinical triage, and the complex implementation paradox facing low-resource regions.
1. The Global Economic Advantage: Reducing the Healthcare Burden
Relying on late-stage cancer treatment instead of proactive screening is financially devastating for any healthcare system. In high-resource settings like the United States, end-of-life care for cervical cancer averages USD 97,000 per patient, far eclipsing the cost of early intervention.

Globally, transitioning to preventative screening yields massive dividends. It is estimated that every USD 1 invested in comprehensive cervical cancer prevention and treatment generates USD 3.20 in economic returns.
However, the current disease and economic burden is alarmingly uneven, heavily impacting regions with lower Socio-Demographic Indices due to limited access to preventative tools. The table below highlights stark regional disparities in prevalence, incidence, and death rates.
Table 1: Regional Epidemiological Burden of Cervical Cancer (Rates per 100,000 women)
| GBD Region |
Age-Standardized Prevalence Rate (ASPR) |
Age-Standardized Incidence Rate (ASIR) |
Age-Standardized Death Rate (ASDR) |
| High-Income North America |
79.24 (73.58 – 85.98) |
12.69 (12.19 – 13.22) |
Well-Controlled / Minimally Expressed |
| Western Europe |
59.03 (56.44 – 61.83) |
8.71 (8.25 – 9.11) |
Well-Controlled / Minimally Expressed |
| High-Income Asia Pacific |
86.28 (82.71 – 89.75) |
11.03 (10.25 – 11.95) |
Well-Controlled / Minimally Expressed |
| Central Europe |
90.48 (80.59 – 100.41) |
15.93 (14.45 – 17.53) |
191.83 (175.35 – 209.14) |
| Eastern Europe |
104.48 (93.46 – 115.16) |
16.49 (14.80 – 18.10) |
Elevated Burden |
| Central Asia |
70.78 (61.74 – 79.91) |
14.17 (12.38 – 15.92) |
213.84 (187.54 – 241.95) |
| South Asia |
63.62 (54.88 – 73.03) |
15.54 (13.47 – 17.71) |
285.98 (247.23 – 325.23) |
| Southeast Asia |
75.11 (63.34 – 87.74) |
15.17 (12.91 – 17.65) |
Elevated Burden |
| North Africa & Middle East |
19.29 (16.43 – 22.81) |
4.72 (4.04 – 5.50) |
80.04 (67.65 – 93.68) |
Note: Data synthesized from global burden analyses tracking demographic and epidemiological shifts up to the early 2020s. Death rates for high-income regions are suppressed in these specific interval extracts due to their statistical minimalization relative to lower-income regions, reflecting successful downstream clinical management.
2. Superiority in Triage: The Clinical and Economic Edge of HPV Testing
For decades, the cytology-based Pap smear was the standard for secondary prevention. Today, the transition to high-performance molecular HPV testing has revolutionized clinical triage.
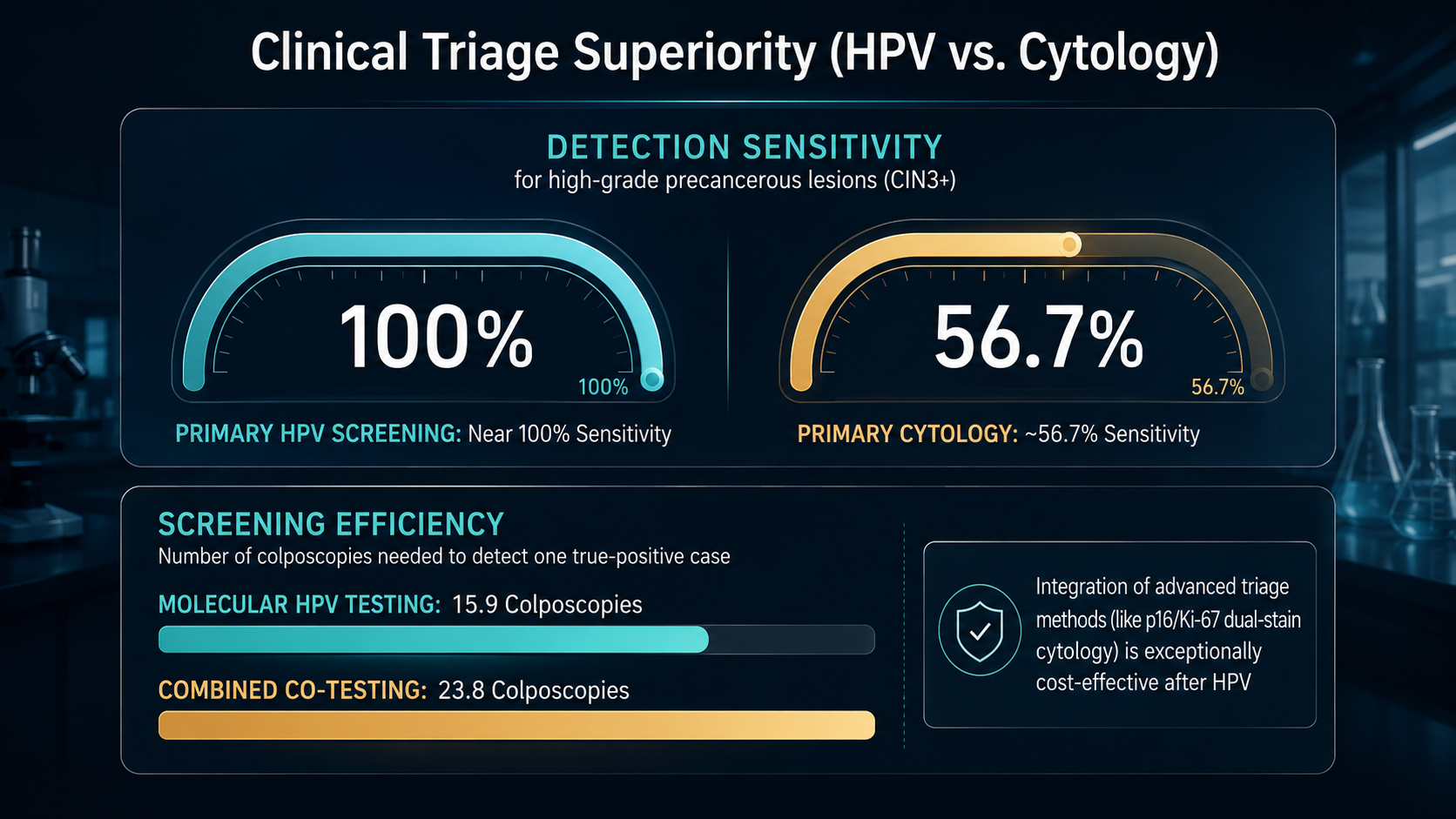
Primary HPV screening boasts near 100% sensitivity for identifying high-grade precancerous lesions (CIN3+), vastly outperforming primary cytology, which traditionally hovers around 56.7% sensitivity. Because molecular testing so accurately intercepts active disease, it requires fewer total colposcopies (15.9) to detect one true-positive case compared to combined co-testing models (23.8).
Furthermore, the integration of advanced triage methods—specifically utilizing p16/Ki-67 dual-stain cytology exclusively for women who initially test positive for high-risk HPV—has proven to be exceptionally cost-effective. This algorithmic triage prevents unnecessary invasive procedures, maximizing health gains while driving down programmatic expenditures. Crucially, the high negative predictive value of an HPV test allows health systems to safely extend screening intervals to 5 years, massively reducing the overall volume of clinic visits and freeing up critical medical capacity.
Global Impact: Easing the Burden on Healthcare Systems
The real-world economic and systemic impact of adopting primary HPV testing with advanced triage mechanisms is being proven across diverse global healthcare frameworks:
- England: Transitioning to HPV primary screening is projected to decrease annual cytology testing volumes by an astounding 2.76 million tests, effectively reducing the overall need for cytology by 80% to 85%. This massive reduction in laboratory workload is estimated to prevent 290 cervical cancer cases and save the National Health Service (NHS) £13 million annually.
- Chile: A comprehensive microsimulation of the Chilean public healthcare system evaluated shifting from cytology every three years to primary high-risk HPV testing every five years. Using a reflex p16/Ki-67 dual-stain triage yielded the greatest health gain (an incremental 13,003 Quality-Adjusted Life Years, or QALYs) while saving $16.65 per woman. Alternatively, reflex cytology triage maximized absolute financial savings at $32.57 per woman. Both strategies were dominant—simultaneously more effective and less costly than the standard of care.
- Thailand: Budget impact modeling for women aged 30–65 demonstrated that HPV primary screening followed by dual-stain triage significantly decreased the prevalence of precancerous lesions and mortality compared to conventional Pap smears. It achieved an Incremental Cost-Effectiveness Ratio (ICER) of just $1,395 per QALY gained, proving highly cost-effective for the Thai healthcare payer.
- Brazil: In a population-based program in Indaiatuba, replacing conventional cytology with high-risk HPV testing algorithms proved to be an economically dominant strategy, generating an economy of US$ 37.87 per QALY gained when utilizing a hybrid cytology triage approach.
3. The LMIC Paradox: Short-Term Strain vs. Long-Term ROI
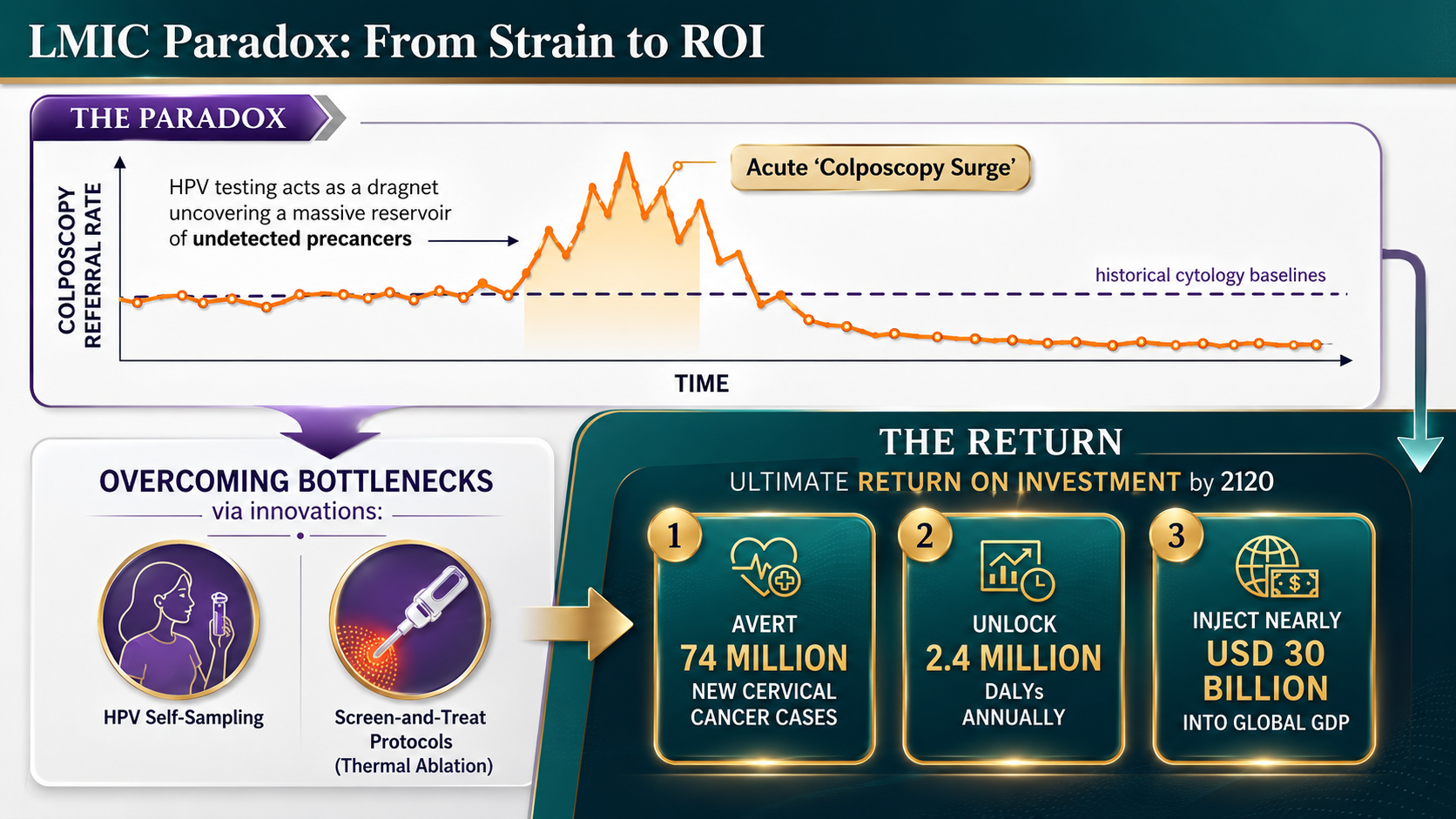
While the economic logic of HPV screening is irrefutable, implementing it in Low- and Middle-Income Countries (LMICs) introduces a daunting paradox. Because HPV testing is so sensitive, rolling it out in historically under-screened populations acts as a dragnet. It immediately uncovers a massive reservoir of previously undetected precancers, triggering an acute “colposcopy surge.”
This sudden spike in required follow-ups and diagnostic biopsies places immense short-term pressure on fragile healthcare systems, often overwhelming the limited availability of trained gynecologists and pathology labs.
Overcoming the Bottleneck
Longitudinal real-world data proves this capacity strain is strictly temporary. After the initial screening rounds successfully clear prevalent precancers, subsequent colposcopy referral rates drop dramatically, eventually falling below historical cytology baselines.
To bypass the immediate infrastructural bottlenecks, global health initiatives are deploying strategic innovations:
- HPV Self-Sampling: Allowing women to collect their own samples in private vastly improves participation rates in rural communities while eliminating the need for a physician-led pelvic exam.
- Screen-and-Treat Protocols: Rather than requiring multiple visits for diagnosis and treatment, women testing positive for HPV are offered immediate thermal ablation in the same clinical encounter, preventing loss-to-follow-up.
The Ultimate Return on Investment
Despite the transitional hurdles, the long-term Return on Investment (ROI) of establishing robust HPV screening in LMICs is phenomenal. Achieving the 2030 WHO elimination targets will not only save lives but will avert an estimated 74 million new cases of cervical cancer by 2120. By keeping women healthy and active in the workforce, this global effort is projected to unlock 2.4 million Disability-Adjusted Life Years (DALYs) annually, injecting nearly USD 30 billion into the global GDP.
As we mark International Women’s Health Day, the message for policymakers is clear: investing in the transition to primary HPV screening is no longer just a medical recommendation—it is one of the most powerful economic growth strategies of the decade.
References
- [1] Canfell, K., et al. (2020). Mortality impact of achieving WHO cervical cancer elimination targets: a comparative modelling analysis in 78 low-income and lower-middle-income countries. The Lancet.
- [2] World Health Organization (WHO). Global Strategy to Accelerate the Elimination of Cervical Cancer as a Public Health Problem.
- [3] Centers for Disease Control and Prevention (CDC). The high cost of cervical cancer care.
- [4] Roche Diagnostics (2025). The economic imperative of cervical cancer elimination: A call to action for healthcare leaders.
- [5] Global, regional, and national epidemiological and economic burdens of cervical cancer from 1991 to 2021. Frontiers in Public Health.
- [6] Global Burden of Disease (GBD) Study. Age-Standardized Incidence and Prevalence Rates for Cervical Cancer by Region.
- [7] Comparison of primary HPV screening, co-testing, and primary cytology for CIN2/3+ detection.
- [8] Cost-effectiveness of primary HPV genotyping and dual-stain or cytology reflex testing versus cytology-based screening for cervical cancer in Chile.
- [9] Cost-effectiveness of human papillomavirus (HPV) primary screening triage with p16/Ki-67 dual stain cytology in Thailand.
- [10] Cost-effectiveness ratio results of modelling cervical cancer screening strategies in a population-based program in Indaiatuba, Brazil. PLOS One.
- [11] Long-term rates of colposcopy referrals after participation in HPV-based screening: The HPV FOCAL trial.
- [12] Digital Colposcopy and Artificial Intelligence as Auxiliary Diagnostic Tools in Low- and Middle-Income Countries.
- [13] Starr, E. (2022). Launching HPV Self-testing Programs in Rural Communities in Low- and Middle-Income Countries. HPV World.
- [14] ASCO. Mozambique as a Case Example of Implementing Cervical Cancer Screening (Screen & Treat protocols in LMICs).
- [15] Public Health England. Clinical impact and cost-effectiveness of primary cytology versus HPV testing in England.
