A literature highlight on the latest diagnostic-care evidence in women’s reproductive health.
Vaginitis is one of the most common reasons women seek gynecological care worldwide. It is also one of the most frustrating: the causes are varied, cure rates are modest, and recurrence is common. For years, clinicians have agreed in principle that accurate diagnosis is the key to better outcomes. But what actually happens in everyday practice — at scale, across millions of real patients?
A recent analysis published in AJOG Global Reports set out to answer exactly that, using real-world data from more than four million patients in the United States. The findings offer a clear, data-driven portrait of where vaginitis care succeeds, where it breaks down, and what could change the picture. Below is a summary of what the study found and why it matters for the future of diagnostics.
What is a real-world study?
Real-world studies (RWS) use routine clinical, claims, and medical-record data to reconstruct how patients are actually diagnosed and treated — the real care pathway, the real disease burden, and the real outcomes.
This is the core difference from a randomized controlled trial (RCT). An RCT tightly controls the setting, the participants, and the intervention to prove whether something works under ideal conditions. A real-world study instead observes large amounts of data from ordinary practice, without altering the care process, to show how well — and how safely — an approach performs across the broad population of everyday patients.
For vaginitis, real-world evidence can reveal what controlled trials cannot: how the condition is actually tested and treated in the clinic, and exactly where the gaps, errors, and pain points lie.
A study of more than four million patients
Using real medical-claims data to trace the full care pathway, the study followed over 18.7 million patients who presented with vaginitis symptoms between 2018 and 2022. After applying the study criteria, 4,000,615 patients were included in the analysis — roughly 3.78 million non-pregnant patients and over 210,000 pregnant patients.
The scale alone confirms what clinicians already sense: vaginitis is a very high-volume, high-recurrence problem and the single most common gynecological complaint in this population.
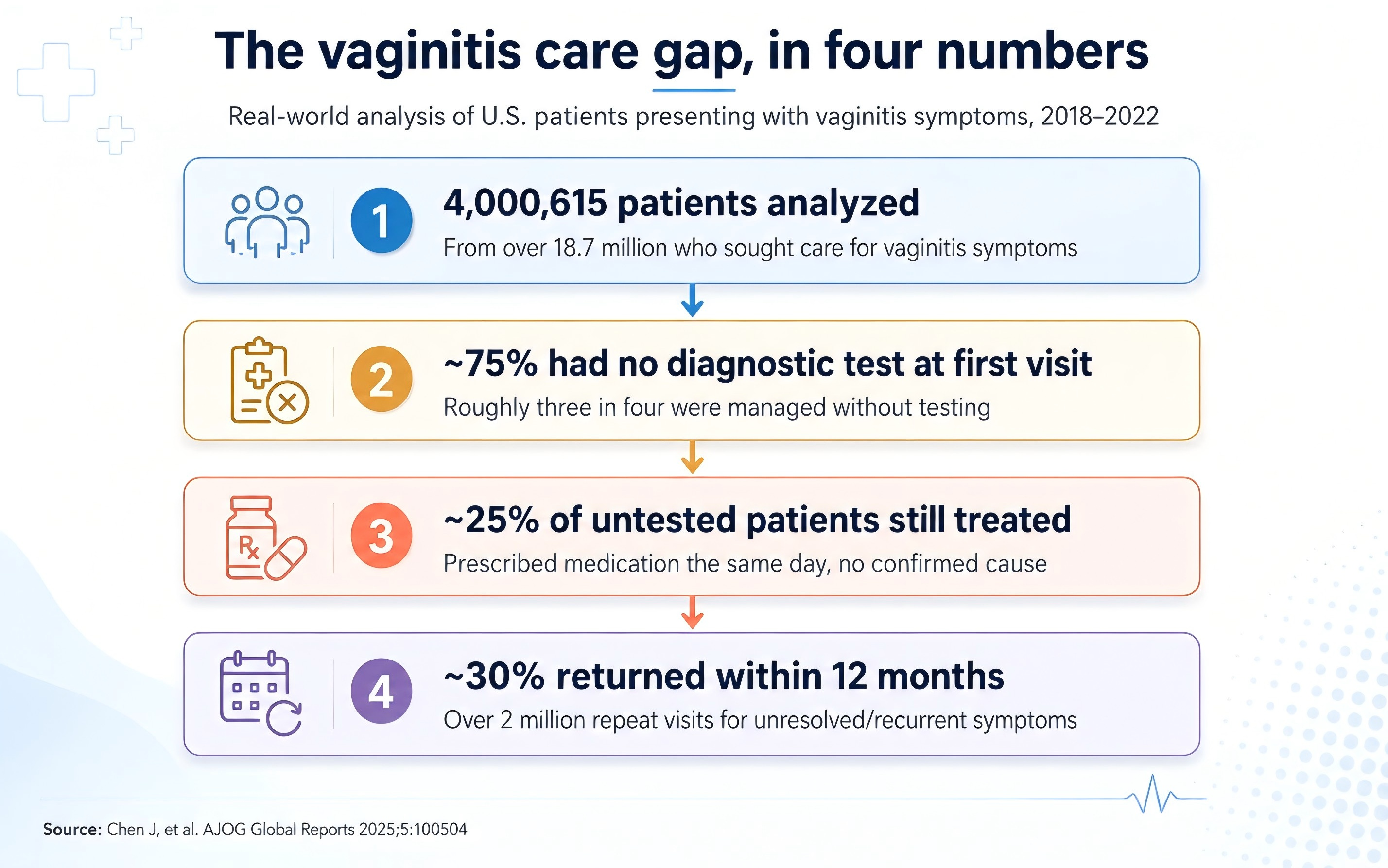
Figure 1. The vaginitis care gap in four numbers.
Finding 1: Testing is badly underused
The study describes the real-world picture of how patients presenting with vaginitis symptoms are managed — at the first visit and across long-term follow-up.
The pattern is striking: a large share of patients are prescribed medication with little or no diagnostic testing, and then return repeatedly for further visits, repeat treatment, and additional care. Across the analytic cohort, roughly three-quarters of patients had no claimed diagnostic test for vaginitis at their initial visit. Among pregnant patients — where accuracy matters most — testing was somewhat more common, with about 47.6% having a claimed test at symptom presentation, but even there, more than half went untested.
When testing did occur, higher-sensitivity, higher-specificity molecular approaches that can distinguish the main causes of vaginitis in a single workup were used in only a minority of cases; traditional methods still accounted for a large share of testing.
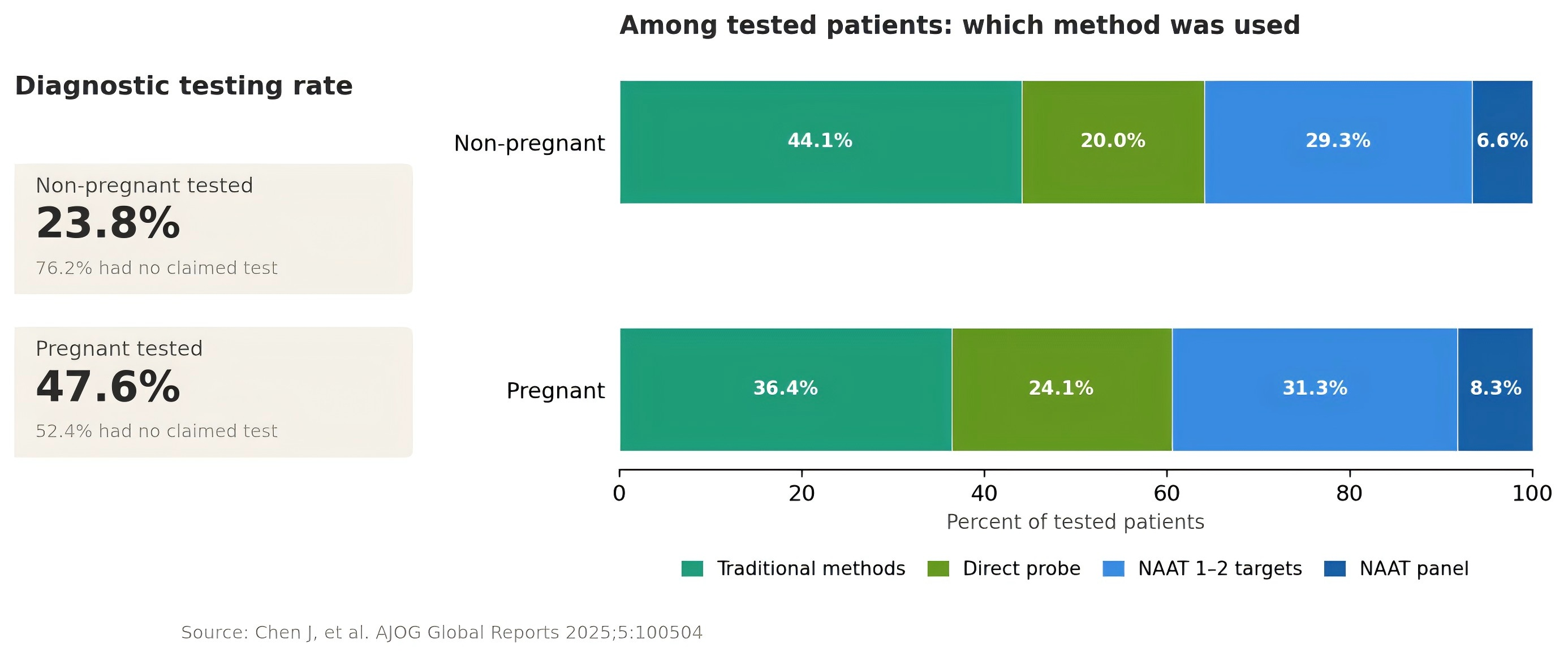
Figure 2. Diagnostic testing rates and method mix among tested patients.
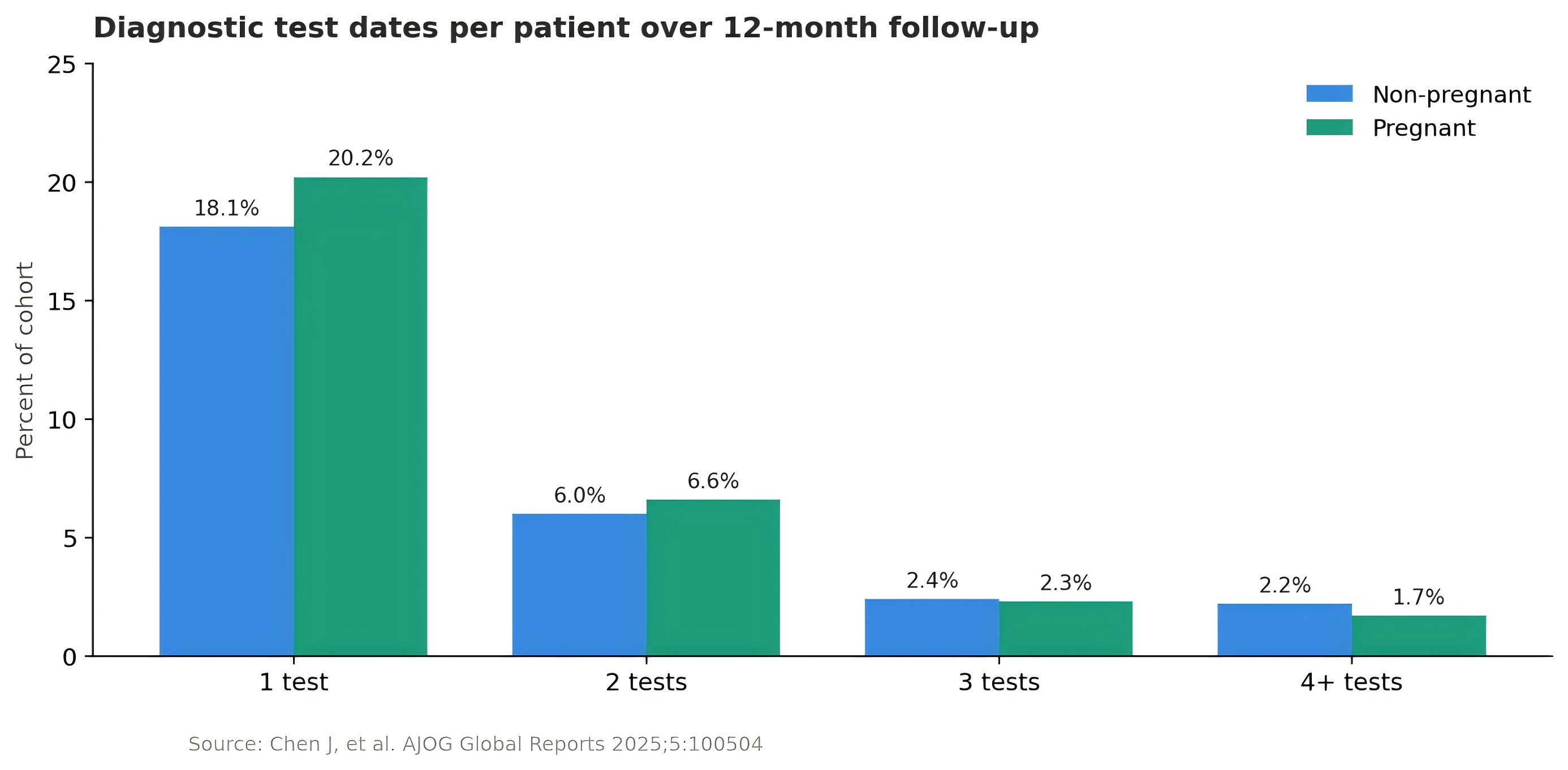
Figure 3. Number of diagnostic test dates per patient over 12-month follow-up.
Finding 2: Empiric prescribing is widespread — and recurrence follows
Despite the low testing rates, prescriptions were issued freely. Among patients with no diagnostic test at their initial visit, roughly one in four were still prescribed vaginitis-related medication on the very same day — treatment without a confirmed cause. Over the full 12-month follow-up, treatment was common in both cohorts, with about 51% of non-pregnant patients and 61% of pregnant patients receiving at least one vaginitis-related treatment.
The consequences showed up downstream. Within 12 months, roughly 30% of the analyzed cohort had at least one vaginitis-related repeat visit because symptoms were unresolved or had recurred — adding up to more than two million repeat visits. The most frequently used treatments during follow-up were a small number of standard agents, notably fluconazole and metronidazole, the kind of repeated, broad empiric use that is widely associated with higher resistance and higher recurrence risk.
In other words: treating without diagnosing does not make the problem go away. It defers it — and often amplifies it.
Finding 3: The burden falls hardest on vulnerable groups
Multivariable analysis comparing patients on public versus commercial insurance found that, after controlling for other factors, publicly insured patients had a 26–27% higher likelihood of repeat visits during follow-up and roughly a 34% higher risk of receiving multiple courses of treatment. Disparities by patient demographics were also significant.
This turns a clinical issue into an equity issue: the populations least able to absorb repeated visits and repeated treatment are the ones most exposed to the consequences of imprecise care.
Three pain points across the whole care pathway
Pulling the findings together, three connected problems emerge:
- Under-diagnosis leads to misdiagnosis and mistreatment. Low testing rates make it hard to tell apart the different causes of vaginitis, raising the risk of the wrong treatment — or no effective treatment at all. For pregnant patients, this also carries downstream risks for pregnancy outcomes.
- Empiric treatment drives both resistance and recurrence. Reaching for the same standard drugs without a confirmed diagnosis blunts effectiveness and contributes to resistant strains, making repeat episodes the norm and adding to patients’ physical, emotional, and financial burden.
- Healthcare resources are wasted, and the burden compounds. With higher repeat-visit and repeat-treatment rates concentrated in vulnerable groups, inefficient care consumes large amounts of resources without delivering the outcomes patients need.
The throughline: diagnose first
The single most consistent signal across more than four million records is simple. The problem is not primarily which test is used — it is that, far too often, no diagnosis is made before treatment begins. More than half of symptomatic patients were prescribed medication without testing, and that upfront gap is what cascades into recurrence, repeat visits, rising resistance, and wasted resources.
Guidance is moving in the same direction. Recent professional recommendations increasingly favor sensitive, specific testing that can identify the main causes of vaginitis — bacterial vaginosis, vulvovaginal candidiasis, trichomoniasis, and mixed infections — in a single workup, so that the right treatment can be matched to the right cause from the first visit.
The promise of “diagnose first” is straightforward: one visit, a confident diagnosis, the right treatment — reducing empiric prescribing at the source, lowering recurrence and repeat visits, and serving both healthcare equity and resource efficiency.
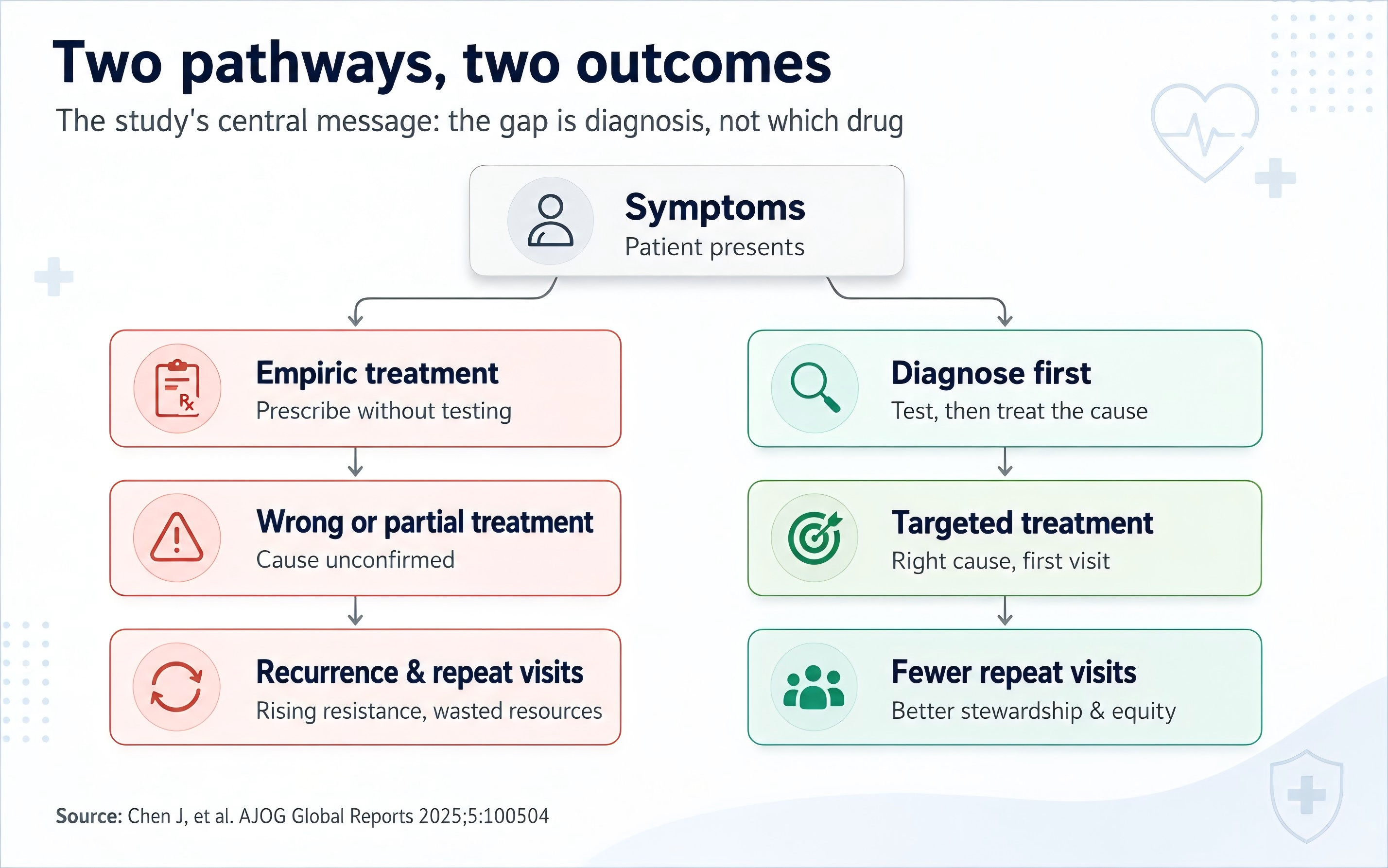
Figure 4. Two care pathways: empiric treatment versus diagnose-first.
Where diagnostics goes from here
For the diagnostics field, this evidence points to a clear direction of travel:
- The standard is rising — from “a test exists” to accurate, fast, and comprehensive diagnosis as the real clinical and patient need.
- Settings are diversifying — care must work across outpatient, urgent, and maternal-health settings, and across higher-risk groups including pregnant and reproductive-age women.
- Value is measurable — precise diagnosis that lowers recurrence, reduces repeat visits, and curbs resistance creates genuine clinical and social value.
In closing
This analysis offers a comprehensive, evidence-based view of how vaginitis is diagnosed, treated, and managed in the real world — and of the disease burden that current practice leaves behind.
Women’s reproductive health is never a small matter, and better vaginitis care begins with a single, decisive step: an accurate diagnosis, made before treatment, every time.
Shared as part of our ongoing literature series on advances in women’s reproductive health diagnostics.
Reference
Chen J, Tse J, Shi L, Cheng MM, Lillis R, Near AM. Real-world clinical burden of patients presenting with vaginitis symptoms in the United States. AJOG Global Reports. 2025;5:100504.
