Two recent publications—a Chinese expert consensus and an international review—are bringing renewed attention to standardized HPV viral load testing as a potential tool for improving cervical cancer screening, risk stratification, and clinical triage.
I. Chinese Expert Consensus on HPV Viral Load for Cervical Cancer Screening and Triage Officially Published
In March 2026, the Chinese Expert Consensus on the Use of Human Papillomavirus Viral Load for Cervical Cancer Screening and Triage was officially published. The consensus was jointly developed by several authoritative academic organizations, including the Colposcopy and Cervical Pathology Branch of the Chinese Eugenics Science Association and the Gynecologic Oncology Branch of the Chinese Medical Association.
The consensus was reviewed and finalized by leading experts in gynecology and laboratory medicine, including Academician Ma Ding, Professor Wei Lihui, Professor Kong Beihua, Professor Xiang Yang, Professor Wang Chuanxin, and Professor Xu Yingchun. It brings together China’s clinical experience and technological innovation in HPV testing for cervical cancer screening.
The key significance of the consensus lies in its direct response to a long-standing technical challenge in HPV viral load quantification: variability in sample collection. In cervical exfoliated cell samples, differences in sampling adequacy and cellularity may affect the interpretation of viral load results. To address this issue, the consensus emphasizes standardized quantitative testing based on quantitative real-time PCR (qPCR), using a human single-copy gene as an internal reference.
This approach enables HPV viral load to be normalized according to the number of human cells in the sample, making results more comparable across samples and time points.
Three Core Points Highlighted in the Consensus
- Standardized quantitative testing: A qPCR-based quantitative method using a human single-copy gene as an internal reference is considered a relatively ideal approach for HPV viral load detection. By correcting for sample cellularity, this method helps reduce sampling bias and improve the comparability of test results.
- A unified clinical threshold: A viral load threshold of ≥4.0 log10 HPV copies per 10,000 cells, equivalent to ≥10,000 HPV copies per 10,000 cells, is recommended as a clinical risk-stratification threshold. This provides a unified reference for interpreting HPV viral load results.
- Defined triage pathways: The consensus proposes clear HPV viral load-based triage pathways for both HPV primary screening-positive populations and populations with abnormal results from combined HPV and cytology screening. This supports the integration of primary screening and triage within a single testing workflow, with the aim of improving screening specificity and reducing unnecessary colposcopy referrals.
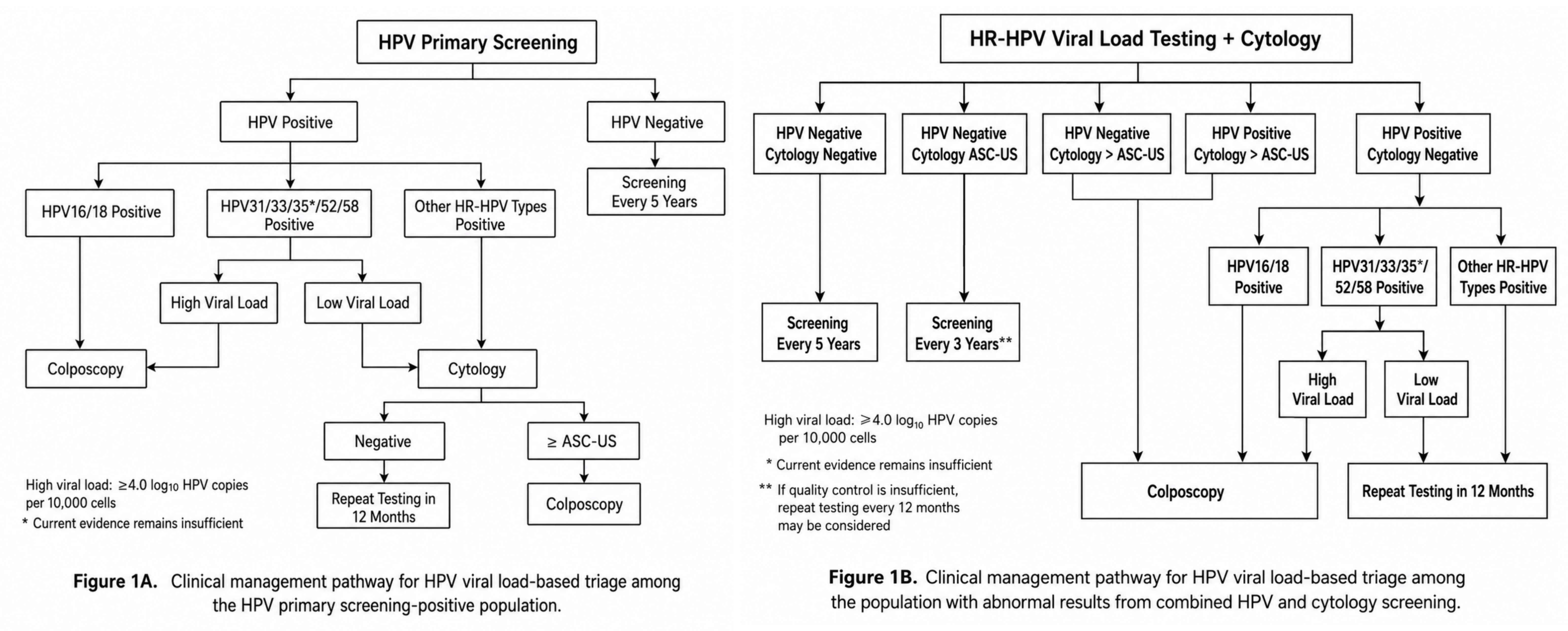
Figure 1. Clinical management pathways for HPV viral load-based triage in cervical cancer screening. Adapted from the Chinese Expert Consensus on the Use of Human Papillomavirus Viral Load for Cervical Cancer Screening and Triage.
By defining a standardized testing method, a clinical threshold, and applicable management pathways, the consensus provides a reproducible and scalable China-based model for cervical cancer screening triage.
II. An International Review Highlights HPV Viral Load as a Promising Surrogate Biomarker
Laurent Bélec and colleagues from the Laboratory of Virology at Hôpital Européen Georges-Pompidou, Assistance Publique–Hôpitaux de Paris, and collaborating institutions recently published a review entitled Human Papillomavirus Viral Load as Promising Surrogate Biomarker of Cervical Cancer Risk and Clinical Outcome in Expert Review of Molecular Diagnostics.
The review discusses HPV viral load as a promising surrogate biomarker for cervical cancer risk and clinical outcomes. Persistent infection with high-risk human papillomavirus (HR-HPV) causes cervical precancerous lesions and cervical cancer. Although molecular HPV DNA testing offers greater sensitivity than cytology as a primary screening method, its limited specificity can lead to unnecessary follow-up procedures. Identifying surrogate biomarkers that can distinguish transient infections from clinically relevant persistent infections is therefore essential for improving risk stratification.
According to the review, oncogenic HPV viral load refers to the quantity of HPV genomes in a sample. Higher viral load levels have been reported to correlate positively with HR-HPV persistence and an increased risk of high-grade lesions and invasive cervical cancer. Viral load quantification may also provide prognostic information regarding disease severity, therapeutic response, and post-treatment recurrence.
Importantly, the review discusses the adoption of standardized and reproducible molecular tools for triaging HPV-positive populations, including comprehensive HR-HPV genotyping and genotype-specific viral load quantification. This approach has the potential to refine risk stratification in cervical cancer screening programs by improving the specificity of HPV-based screening beyond the simple detection of viral DNA.
The review presents the BioPerfectus Multiplex Real-Time (BMRT) HPV Genotyping PCR Kit, developed by Jiangsu Bioperfectus Technologies Co., Ltd., China, as an example of standardized HPV viral load measurement.
III. Standardized Quantification Corrected by an Internal Reference Gene
HPV viral load testing has evolved from semi-quantitative methods to standardized quantitative approaches.
Early methods, such as nested PCR combined with probe hybridization, enabled semi-quantitative detection of viral DNA but had limitations in sensitivity and clinical practicality. Southern blotting could distinguish episomal viral DNA from integrated viral DNA, but it was less convenient than PCR for routine use. Hybrid Capture 2 (HC2) later became a validated method for detecting HR-HPV DNA, but it provides pooled HR-HPV detection rather than type-specific viral load and is considered semi-quantitative.
The development of quantitative real-time PCR represented a major advance. qPCR enables the precise amplification of specific viral DNA fragments and supports genotype-specific detection and quantification. However, early HPV viral load studies often relied on HC2 signal intensity or PCR cycle threshold values, typically without standard-curve calibration or normalization to the number of cervical exfoliated cells in the specimen.
To address the inherent variability of genital sampling, recent studies have used qPCR assays targeting housekeeping genes as internal controls. Examples include human genomic DNA targets such as β-globin, CCR5, ERV-3, and TOP3. These internal controls can verify DNA extraction quality, confirm sample integrity, detect potential PCR inhibitors, and enable normalization of viral load according to the cellular content of the sample.
By expressing HPV viral load as copies per cell equivalent, the intrinsic variability and differences in specimen cellularity associated with genital sampling can be partly controlled. The review describes this approach as a recognized standard in molecular virology for non-fluid-based samples because it enables standardized comparisons between patients beyond the physical volume of the original swab specimen.
TOP3-Based Cellularity Assessment in the BMRT Workflow
In the BMRT-based workflow discussed in the review, TOP3 is used as a human single-copy gene internal reference. The TOP3 gene serves as a sample adequacy control for cell quantification. HPV DNA and TOP3 are amplified within the same overall quantitative workflow, allowing the resulting HPV viral load to be expressed relative to the number of human cells in the sample.
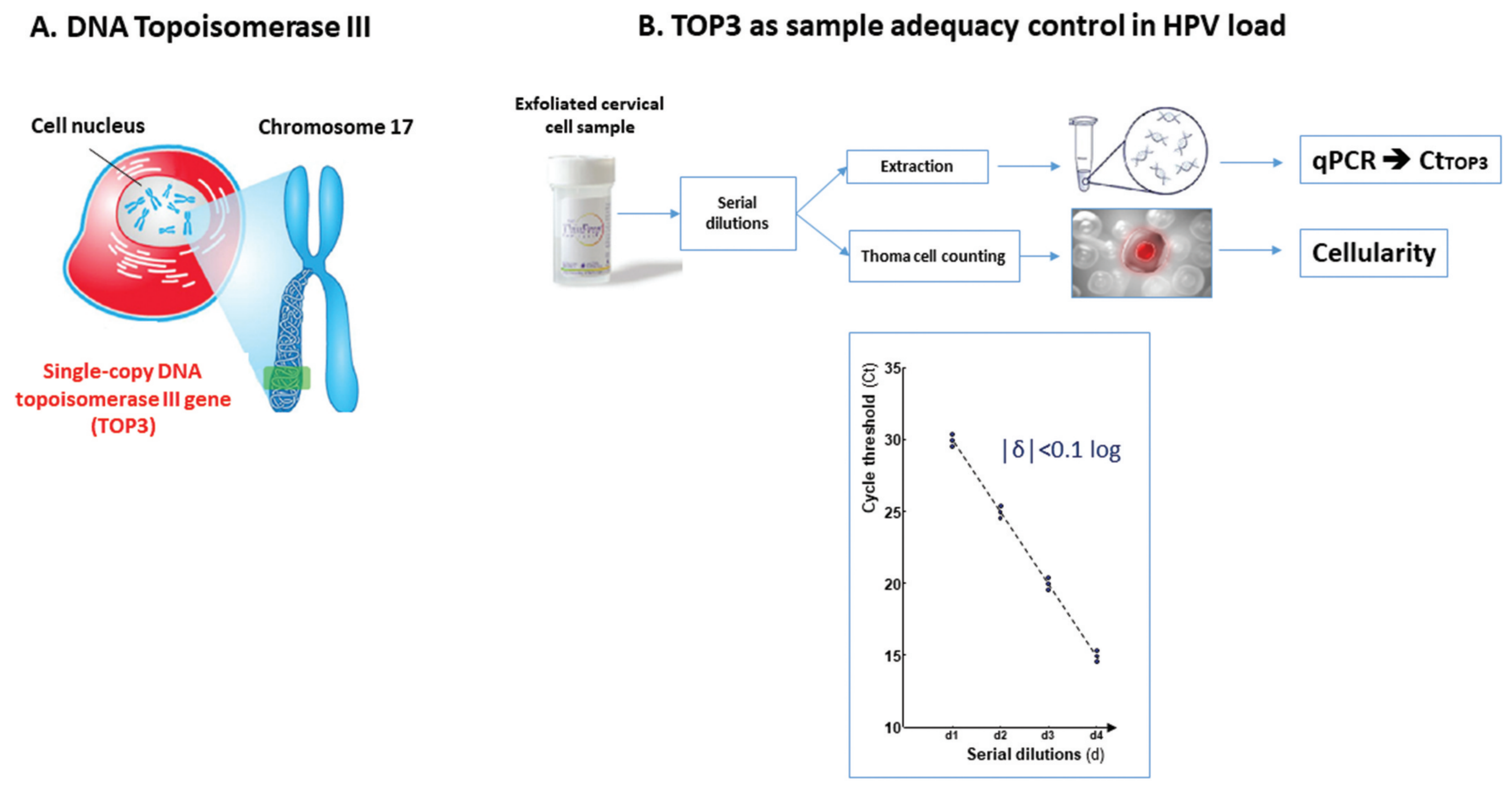
Figure 2. TOP3-based cellularity assessment and sample adequacy control in the BioPerfectus BMRT HPV Genotyping Real-Time PCR workflow. A. TOP3, a well-conserved human single-copy gene located on chromosome 17, is used as a cellular internal control to assess human DNA content, sample cellularity, and sample adequacy. Its amplification provides a molecular reference for human cell quantification and helps account for variability introduced during sample collection, DNA extraction, and PCR. B. During assay verification, cervical exfoliated cell samples were serially diluted and evaluated in parallel using microscopy-based hemocytometer counting and TOP3 cycle threshold measurements. The two approaches showed close agreement, with a variation of |δ| <0.1 log, supporting the reliability of TOP3-based quantification of human nucleated cells in cervical samples.
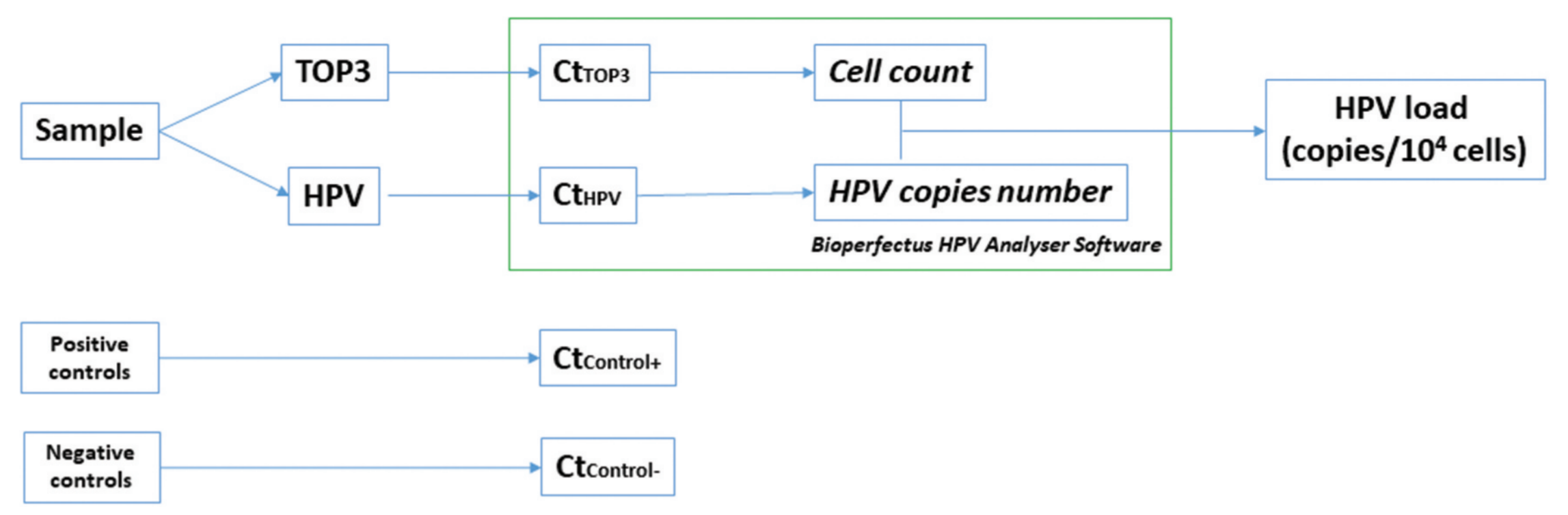
Figure 3. Standardized HPV viral load quantification using the BioPerfectus BMRT HPV Genotyping Real-Time PCR Kit. Each clinical sample is simultaneously tested for HPV DNA and the human single-copy gene TOP3. The cycle threshold values for HPV and TOP3 are analyzed by BioPerfectus HPV Analyser Software to calculate HPV copy number and human cell count, respectively. Positive and negative controls are included to verify amplification performance and assay reliability. The resulting HPV viral load is normalized to the cellular content of the sample and reported as HPV copies per 10,000 human cells or as log10-transformed copies per 10,000 cells. This approach supports accurate, reproducible, and comparable viral load measurement across samples by accounting for differences in sample cellularity and collection efficiency.
In standardized reporting, HPV viral load is commonly expressed as copies per 10,000 cells or as log10-transformed copies per 10,000 cells. This format provides a more biologically meaningful and comparable measure of viral burden than reporting viral copies per unit volume because it accounts for variations in sample collection efficiency and cellularity.
IV. ROC Curve Analysis for Determining Clinically Relevant Cutoff Values
The review further discusses the use of receiver operating characteristic (ROC) curves to determine optimal HPV viral load cutoff values. ROC curve analysis evaluates the discriminatory capacity of a test by plotting sensitivity, or the true-positive rate, against 1-specificity, or the false-positive rate, across different cutoff points for a continuous variable such as HPV viral load.
Each point on the ROC curve represents a viral load cutoff and reflects the trade-off between sensitivity and specificity. The area under the curve (AUC) summarizes overall diagnostic performance and indicates how effectively viral load, either alone or in combination with other factors, predicts disease progression.
Reported Cutoff Values and Diagnostic Performance
In one study cited in the review, type-specific HR-HPV viral load for detecting high-grade squamous intraepithelial lesions or worse (≥HSIL) achieved an AUC of 0.90. The optimal cutoff was 3.17 log10 copies per 10,000 cells, corresponding to 84% sensitivity and 81% specificity.
Using the BMRT HPV Genotyping PCR Kit, optimal viral load cutoffs were identified for triaging ≥HSIL in HPV-positive populations:
- HPV-16: An optimal cutoff of 4.26 log10 copies per 10,000 cells yielded 79% sensitivity and 81% specificity.
- HPV-31: A cutoff of 4.46 achieved 89% sensitivity and 89% specificity.
- HPV-33: A cutoff of 4.48 provided 83% sensitivity and 83% specificity.
These findings indicate that the BMRT HPV real-time PCR viral load assay can support the clinical triage of ≥HSIL when appropriate cutoff levels are used. The review also notes that such thresholds may guide tailored clinical decision-making and management by helping determine which patients require immediate colposcopy and which may be suitable for reflex testing or safe monitoring.
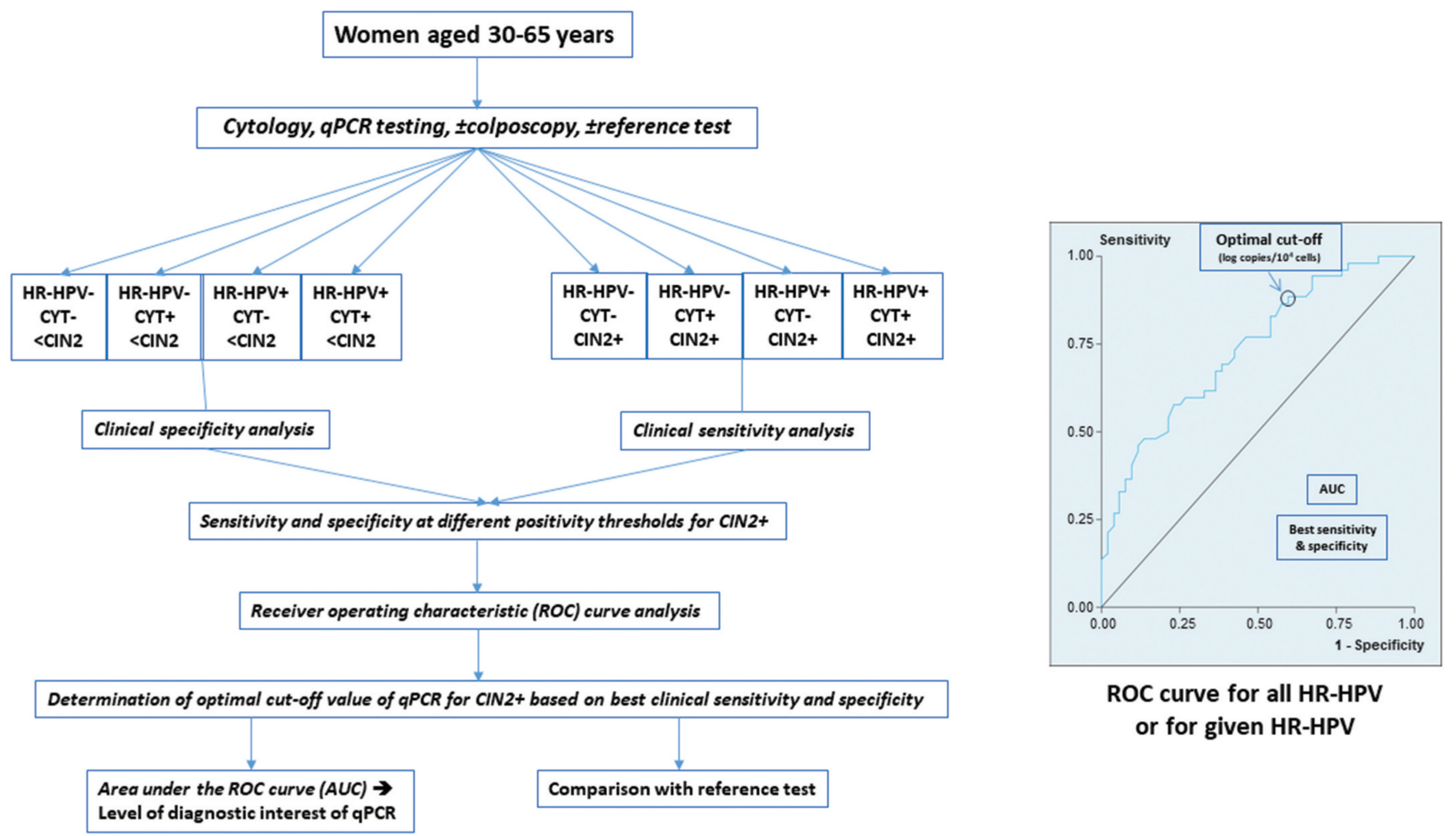
Figure 4. Diagnostic workflow and ROC analysis for qPCR-based detection of CIN2+ in women aged 30–65 years. Following cytology, qPCR testing, and, where applicable, colposcopy and reference testing, participants are stratified according to HR-HPV status, cytology results, and CIN2+ status. Clinical sensitivity and specificity are evaluated across different qPCR positivity thresholds using receiver operating characteristic curve analysis. The optimal cutoff is selected according to the best balance between sensitivity and specificity, while the AUC reflects the overall ability of the test to distinguish between cases and controls.
Abbreviations: AUC, area under the curve; CIN2+, cervical intraepithelial neoplasia grade 2 or higher; Ct, cycle threshold; HR-HPV, high-risk human papillomavirus; qPCR, quantitative real-time PCR; ROC, receiver operating characteristic.
Beyond threshold determination, ROC-derived viral load cutoffs may contribute to risk stratification and improved triage. BMRT HR-HPV viral load combined with genotyping has been described as a valuable secondary strategy for cervical cancer screening, particularly in settings with limited cytological resources. qPCR-based HPV viral load determination may also be particularly valuable for self-collected samples, for which traditional cytology may not be available, potentially enabling immediate risk-based triage.
V. From China to the World: Advancing the Discussion on Cervical Cancer Screening Strategies
The global landscape of cervical cancer prevention has undergone a major transformation, shifting from traditional cytology-based screening toward more sensitive HPV-based molecular screening. HPV DNA testing is recommended by the World Health Organization as a primary screening method because of its higher clinical sensitivity. However, HPV DNA testing alone may have limited specificity and cannot always distinguish transient infections from clinically relevant persistent infections.
This creates what the review describes as a “necessary but insufficient” paradox. HPV infection is necessary for cervical carcinogenesis, but HPV positivity alone is insufficient to determine which infections are likely to progress. Because most HPV infections resolve spontaneously and only a minority progress to CIN3 or worse, complementary biomarkers are needed to reduce overtreatment while maintaining rigorous monitoring of high-risk individuals.
In this context, extended HR-HPV genotyping combined with standardized viral load quantification may provide a more precise approach to cervical cancer screening triage. By integrating genotype-specific risk information with quantitative viral burden, this strategy may help improve clinical specificity, reduce unnecessary colposcopy referrals, and support more personalized follow-up.
The publication of the Chinese expert consensus and the international review in Expert Review of Molecular Diagnostics reflects the growing interest in standardized HPV viral load testing. Together, they also demonstrate how China’s clinical evidence and molecular diagnostic innovation are contributing to the broader global discussion on risk-based cervical cancer screening.
At the same time, this field must be interpreted with scientific rigor. The review notes that HPV viral load remains a promising biomarker, particularly when combined with HPV genotyping, but broader clinical application still requires further standardization, prospective validation, reproducibility assessment, and confirmation of clinical benefit across diverse populations and healthcare settings.
VI. Conclusion: Standardized Quantitative Molecular Diagnostics Supporting Precision Triage
From the Chinese expert consensus to the international review, HPV viral load-based triage is gaining increasing attention as a potential strategy for improving cervical cancer screening specificity and risk stratification.
Both publications emphasize the importance of standardized quantitative testing based on real-time PCR and correction for sample cellularity. By normalizing HPV viral load according to the number of human cells, standardized qPCR-based methods can reduce sampling bias and improve comparability across samples. When combined with extended HR-HPV genotyping, viral load assessment may help identify higher-risk populations, guide colposcopy referrals, support safe follow-up, and reduce unnecessary procedures.
Looking ahead, further real-world evidence, multicenter validation, and internationally harmonized standards will be essential to define the role of HPV viral load in cervical cancer screening programs. With continued innovation in molecular diagnostics, standardized HPV viral load testing may help support more precise, efficient, and accessible screening strategies, contributing to the global goal of cervical cancer elimination.
References
[1] Ralph-Sydney Mboumba Bouassa, Jonathan Muwonga Tukisadila, Hugues Loemba, and Laurent Bélec. Human papillomavirus viral load as promising surrogate biomarker of cervical cancer risk and clinical outcome. Expert Review of Molecular Diagnostics. 2026;26(6):501–522.
[2] Colposcopy and Cervical Pathology Branch of the Chinese Eugenics Science Association; Gynecologic Oncology Branch of the Chinese Medical Association; Female Reproductive Tract Disease Branch of the Chinese Eugenics Science Association; Chinese Maternal and Child Health Association Cervical Cancer Prevention and Control Research Committee. Chinese Expert Consensus on the Use of Human Papillomavirus Viral Load for Cervical Cancer Screening and Triage [in Chinese]. Chinese Journal of Clinical Obstetrics and Gynecology. 2026;27(2):179–185.
