As the Southern Hemisphere enters its high-incidence winter respiratory season, healthcare networks are experiencing a complex resurgence of acute respiratory tract infections (ARIs). The cessation of pandemic-era mitigation strategies has left populations with an “immunity debt,” contributing to the simultaneous co-circulation of SARS-CoV-2, influenza A and B, respiratory syncytial virus (RSV), and other opportunistic respiratory pathogens.
For healthcare providers, medical distributors, and public health officials, understanding these shifting trends is critical to deploying effective clinical strategies. Below is a concise breakdown of the current epidemiological landscape, its economic toll, and the advanced molecular diagnostic tools required to meet this winter challenge.
1. The Epidemiological Shift: A Shifting Winter Respiratory Season
Recent data across Oceania, South America, and Africa show that current respiratory seasons are defying historical predictive models. Pathogen circulation is marked by unseasonably early onsets, dual-wave infection peaks, and genetically drifted strains capable of evading prior immunity.
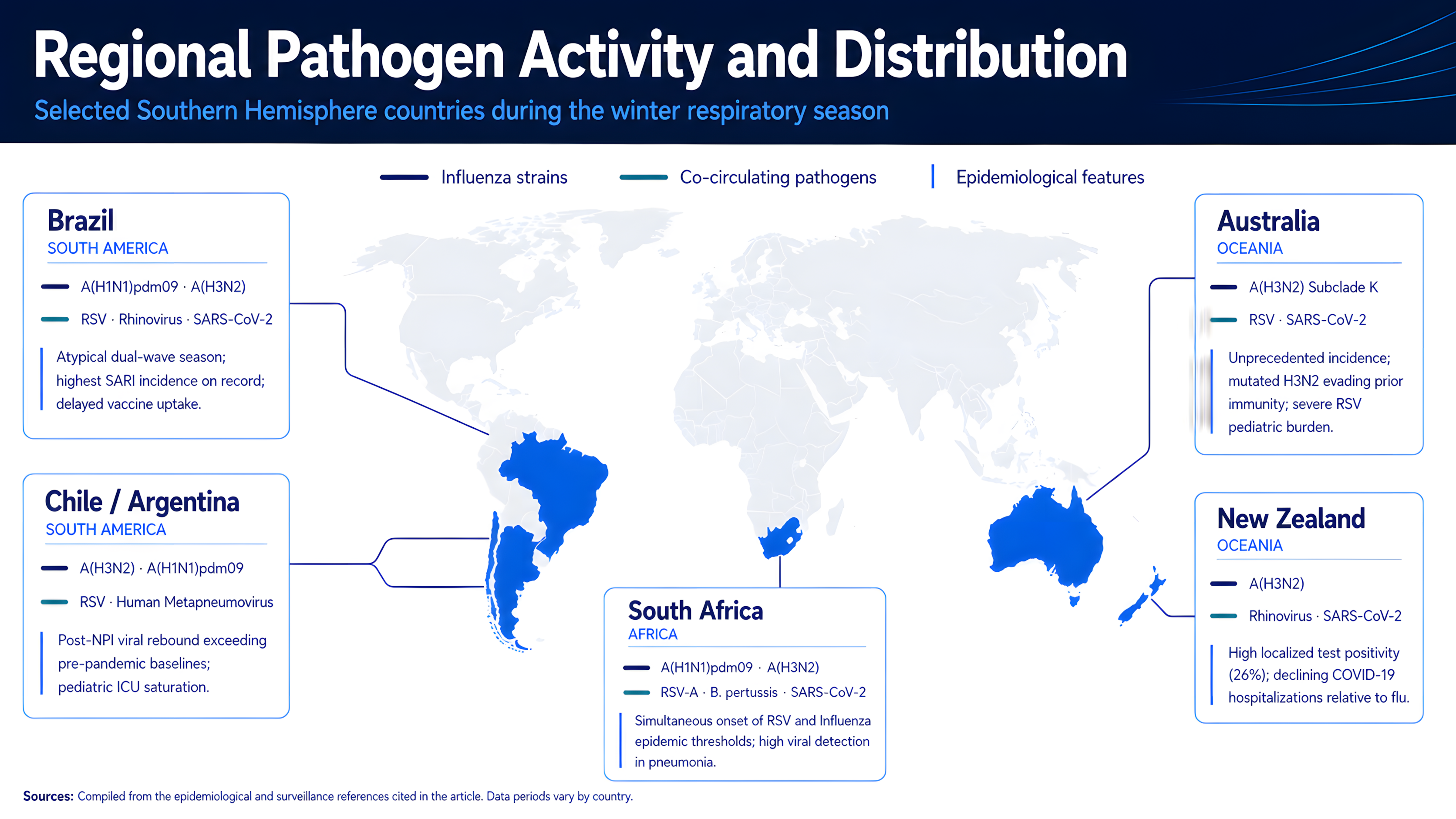
Figure 1. Regional distribution of predominant influenza strains and co-circulating respiratory pathogens across selected Southern Hemisphere countries.
2. The Regional Economic Burden
The concurrent circulation of these respiratory pathogens exerts a substantial economic burden on national healthcare systems and households alike, driven by intensive care unit (ICU) admissions, mechanical ventilation, and workplace absenteeism.
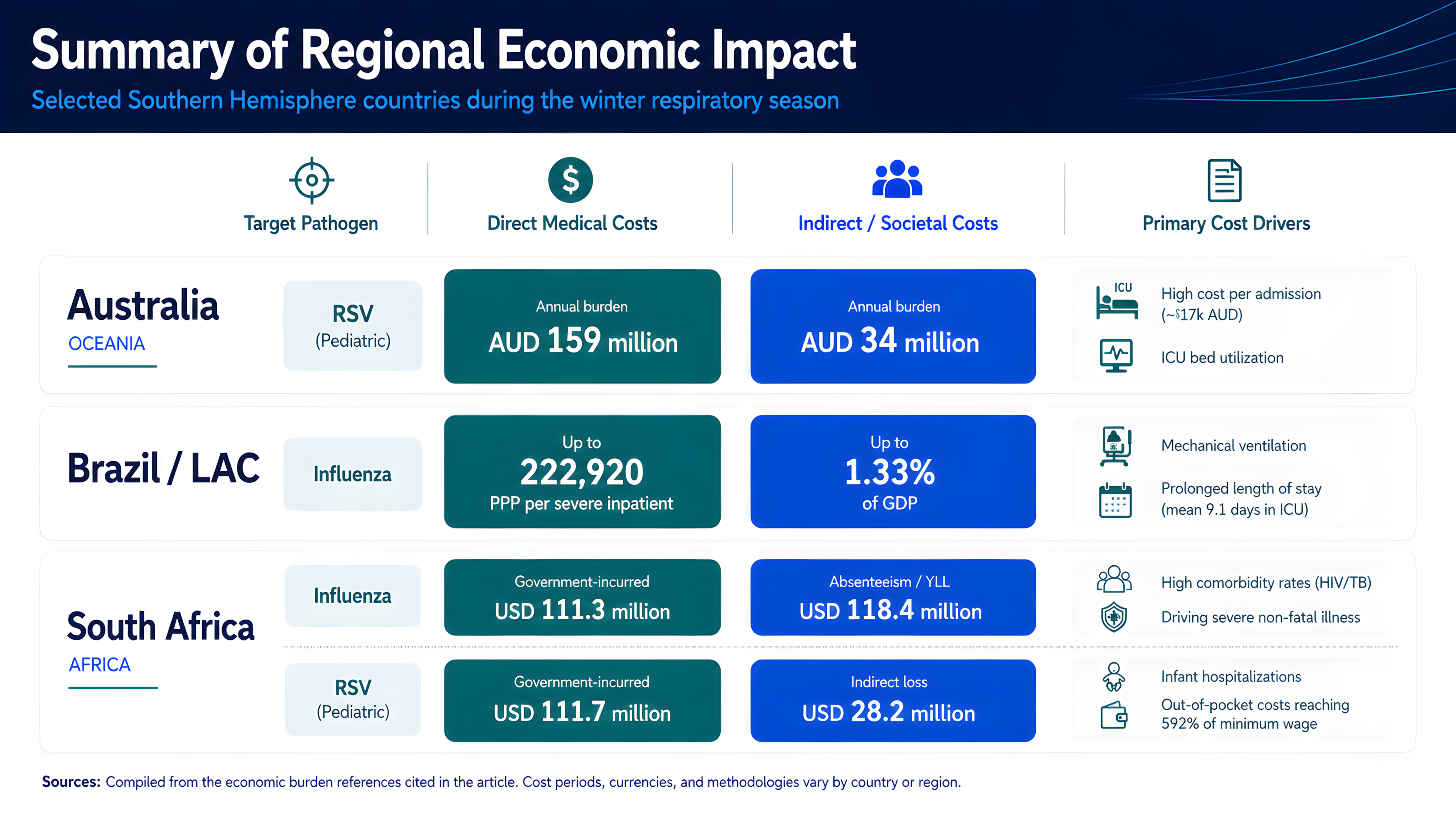
Figure 2. Reported direct and indirect economic burden associated with selected respiratory pathogens across key Southern Hemisphere settings.
3. The Diagnostic Gap: Why Rapid Antigen Tests Fall Short
Traditional, symptom-based clinical triage is largely ineffective because the overlapping clinical presentations of these pathogens often look nearly identical. While rapid antigen lateral flow assays are widely accessible, reliance on antigen-only testing presents important limitations in the current epidemiological environment.
- Low sensitivity: Rapid antigen tests may yield false negatives, particularly during the early or late stages of viral shedding or in elderly populations with lower viral titers.
- Limited scope: Basic single- or dual-target antigen tests do not detect pathogens outside their target scope, including RSV, human metapneumovirus, or secondary bacterial infections.
- Impact on antibiotic stewardship: Diagnostic uncertainty can contribute to empirical over-prescription of broad-spectrum antibiotics for viral conditions, inadvertently accelerating antimicrobial resistance (AMR).
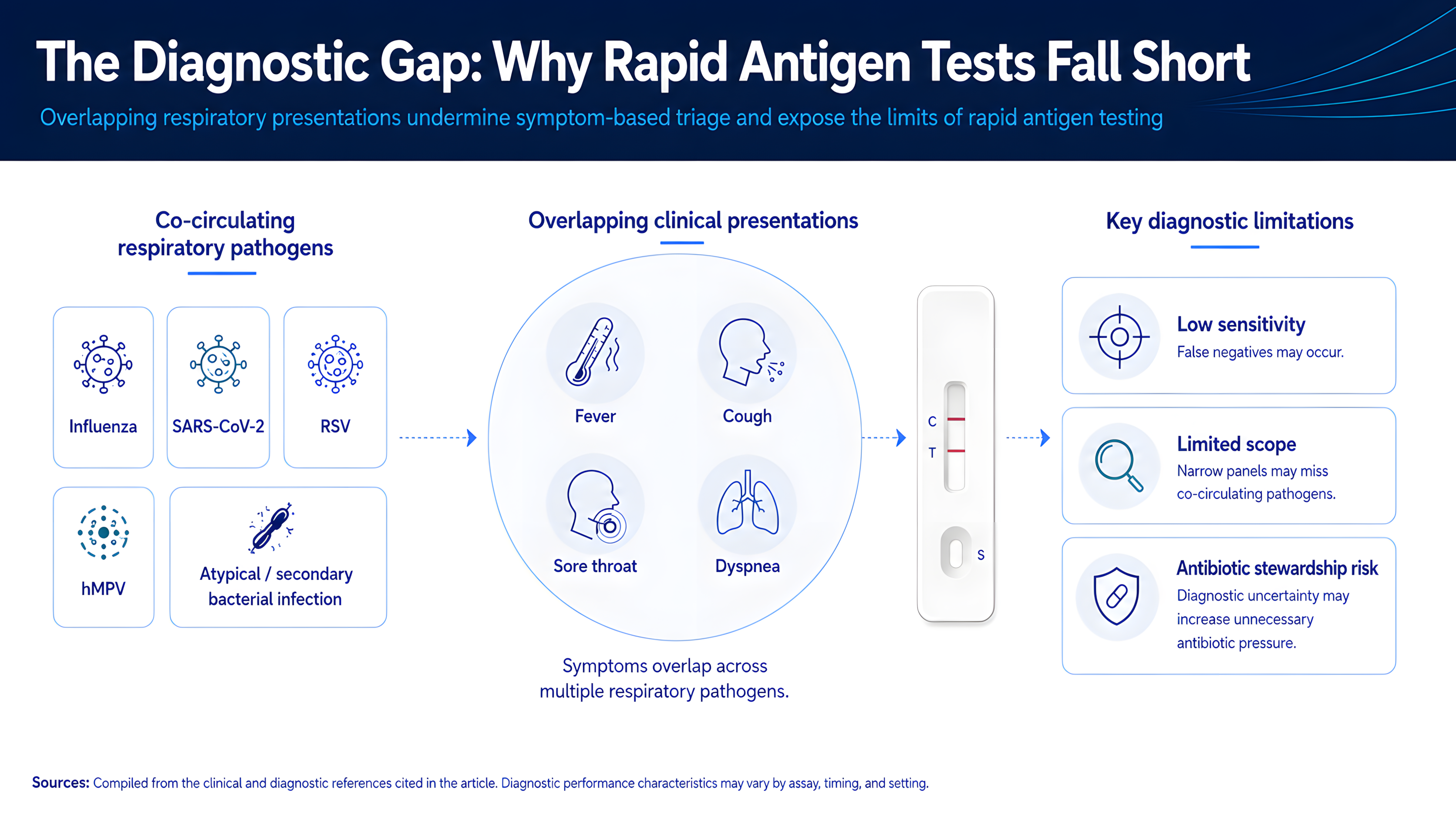
Figure 3. Key diagnostic limitations of rapid antigen testing in high respiratory pathogen co-circulation settings.
4. The Solution: BioPerfectus Advanced Pathogen Profiling
To address the winter respiratory surge, healthcare infrastructures require rapid, highly multiplexed molecular syndromic testing. By amplifying nucleic acids, molecular platforms provide high analytical sensitivity and support pathogen-specific differentiation within defined laboratory workflows.
The BioPerfectus Allfastra series and its comprehensive real-time PCR respiratory panels offer high-throughput, CE-IVD marked solutions designed to support rapid detection of specific respiratory pathogen panels.
- Target pathogens: SARS-CoV-2 (ORF1ab/N/E genes), Influenza A (M gene), Influenza B (NS gene), and Respiratory Syncytial Virus (RSV, N gene).
- Testing relevance: Supports differentiation of four major viral drivers of severe winter morbidity, processing up to 48 specimens in 48 minutes with a limit of detection (LoD) of 200 copies/mL.
- Target pathogens: Influenza A virus, Influenza B virus, Respiratory syncytial virus (RSV), Human rhinovirus, Respiratory adenovirus, Mycoplasma pneumoniae, and Parainfluenza virus.
- Testing relevance: Provides broader respiratory pathogen coverage, including major viral pathogens and atypical bacteria such as Mycoplasma pneumoniae, with results in 72 minutes.
- Target pathogens: Haemophilus influenzae, Mycoplasma pneumoniae, Legionella pneumophila, Klebsiella pneumoniae, Streptococcus pneumoniae, Bordetella parapertussis, and Bordetella pertussis.
- Testing relevance: Supports molecular detection of community-acquired pneumonia (CAP)-related and pertussis-associated bacterial pathogens in 46 minutes with a sensitive LoD of 5 copies/reaction.
- Target pathogens: Pseudomonas aeruginosa, Group A Streptococcus, and Staphylococcus aureus.
- Testing relevance: Supports molecular detection of selected bacterial superinfection markers, helping laboratories reduce diagnostic uncertainty compared with culture-based workflows.
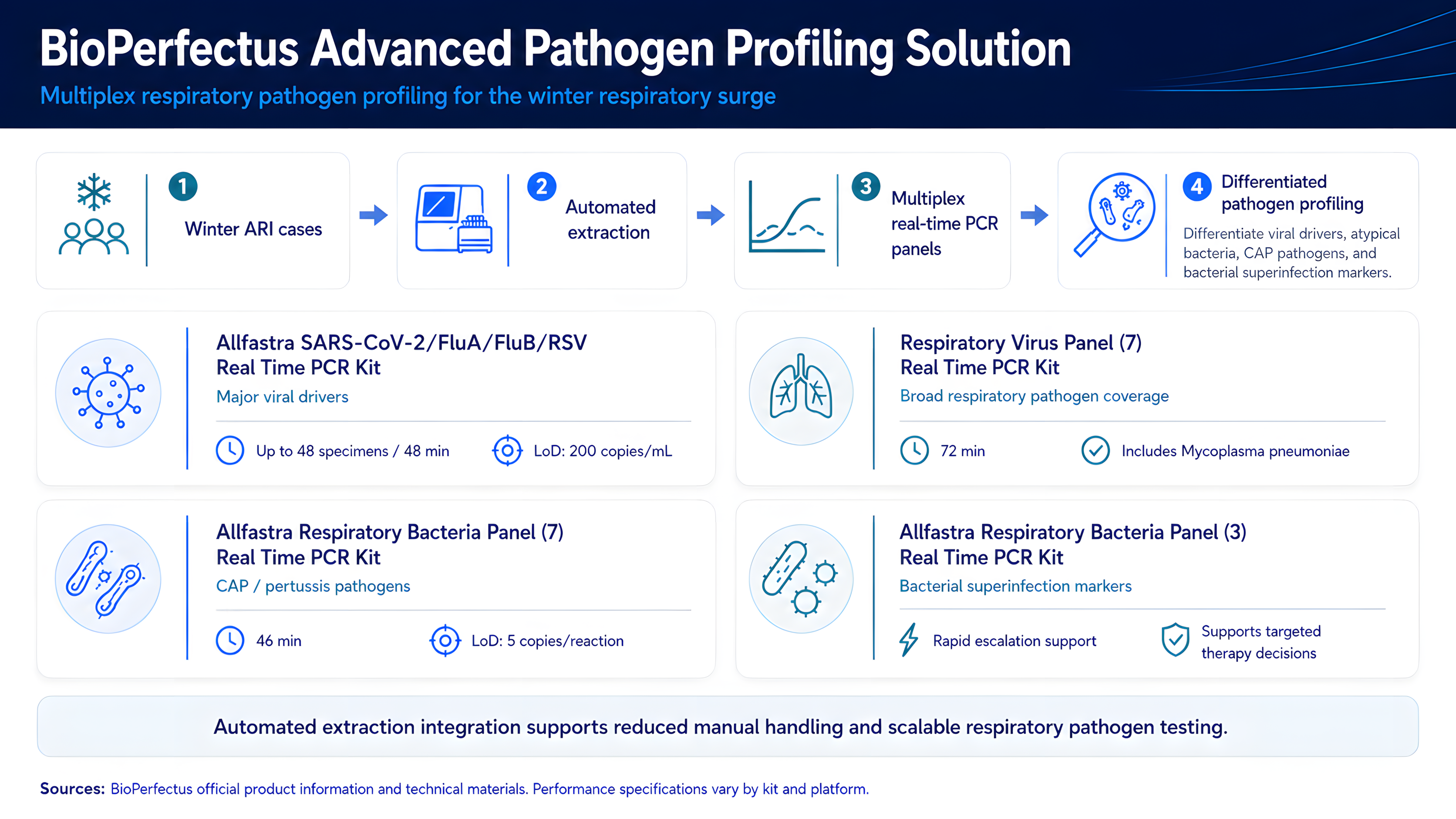
Figure 4. BioPerfectus multiplex respiratory pathogen profiling workflow and product portfolio for broader respiratory pathogen detection.
To minimize manual handling and scale processing capacity, these kits can integrate with BioPerfectus automated nucleic acid extraction workstations, such as the SSNP-2000B and the fully automated walk-away SAW-48/96 platforms. These total PCR solutions support scalable respiratory pathogen testing and preparedness across healthcare networks.
References
Epidemiology and Surveillance
- World Health Organization. (2025). Seasonal influenza: Global situation.
- World Health Organization Western Pacific Region. (2026). Respiratory viruses surveillance bulletin: Epidemiological week 1, 2026.
- Ministério da Saúde. (2026). Informe epidemiológico: Semana epidemiológica 15 de 2026 [Epidemiological report].
- National Institute for Communicable Diseases. (n.d.). Weekly respiratory pathogens surveillance reports.
- National Institute for Communicable Diseases. (2026). 2026 RSV and influenza season alert.
- Ministerio de Salud de Argentina. (2026). Actualización del Boletín Epidemiológico Nacional de la semana N° 22.
- Pacheco, N., Hidalgo, A. A., Gonzalez, R. I., et al. (2025). Epidemiological surveillance and incidence of respiratory viruses in Chile: Before and after COVID-19. Infectio, 29(2), 68–76.
- The Guardian. (2026, June 7). Australia’s winter illness season is back: What viruses are prevalent this year and when should you get vaccinated? The Guardian.
Economic Burden
- Brusco, N. K., Alafaci, A., Tuckerman, J., Frawley, H., Pratt, J., Daley, A. J., Todd, A. K., Deng, Y.-M., Subbarao, K., Barr, I., & Crawford, N. W. (2022). The 2018 annual cost burden for children under five years of age hospitalised with respiratory syncytial virus in Australia. Communicable Diseases Intelligence, 46.
- Tempia, S., Moyes, J., Cohen, A. L., Walaza, S., Edoka, I., McMorrow, M. L., Treurnicht, F. K., Hellferscee, O., Wolter, N., von Gottberg, A., et al. (2019). Health and economic burden of influenza-associated illness in South Africa, 2013–2015. Influenza and Other Respiratory Viruses, 13, 484–495.
- Alvis-Zakzuk, N. J., Couto, P., Jara, J. H., et al. (2025). Economic burden of respiratory viruses in Latin America and the Caribbean (LAC): A scoping literature review. Influenza and Other Respiratory Viruses, 19(9), e70148.
- IQVIA, Global Coalition on Aging, & GSK. (2024). Economic burden of respiratory syncytial virus infection among older adults in select APEC countries.
Diagnostic Testing and Antimicrobial Stewardship
- Damhorst, G. L., & Lam, W. A. (2025). Point-of-care and home-use influenza diagnostics for advancing therapeutic and public health strategies. The Journal of Infectious Diseases, 232(Supplement_3), S314–S326.
- Dickson, E. M., Zambon, M., Pebody, R., et al. (2020). Do point-of-care tests (POCTs) offer a new paradigm for the management of patients with influenza? Eurosurveillance, 25(44), 1900420.
- Hoang, U., Smylie, J., Button, E., Macartney, J., Okusi, C., Byford, R., Ferreira, F., Xie, C., Joy, M., Clark, T., & de Lusignan, S. (2025). The impact of point-of-care testing for influenza on antimicrobial stewardship in UK primary care: Nested cohort study. JMIR Public Health and Surveillance, 11, e72322.
